
Salutogenic Medicare:
Beyond Prevention: Reimagining the Medicare Annual Wellness Visit as a Platform for Late-Life Health Creation

Opening thesis
A 78-year-old Medicare beneficiary comes in for an Annual Wellness Visit. The forms are completed. Medications are reviewed. Falls, depression, cognition, and preventive screenings are discussed. A printout is generated with reminders about vaccines and tests. On paper, the system has done what it was designed to do.
But step back and ask a different set of questions.
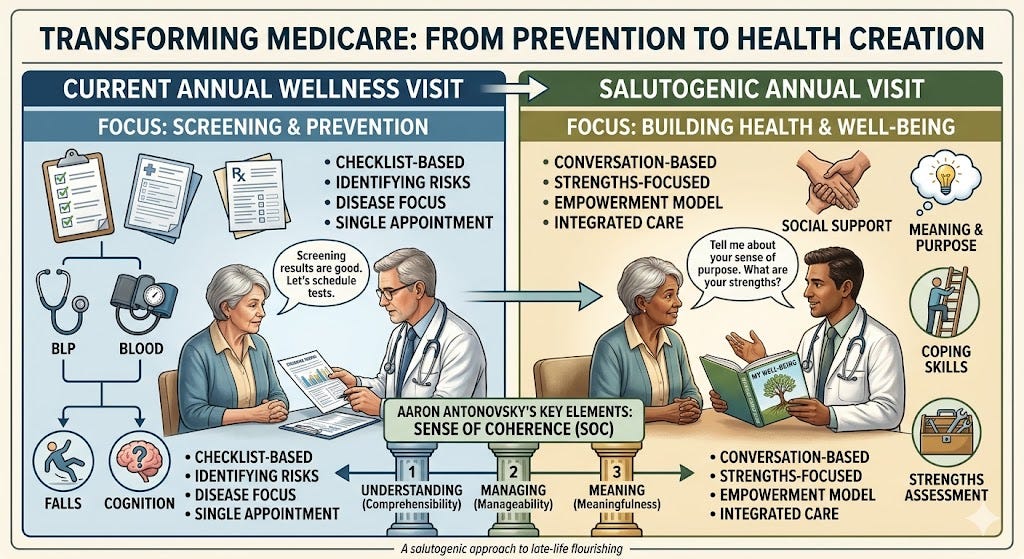
Does this person understand what is happening to their health in a way that feels coherent rather than confusing? Do they have the emotional, social, practical, and financial resources to manage what lies ahead? Do they still experience life as meaningful enough to invest in the work of staying well?
Those questions matter enormously in later life, yet they remain secondary in Medicare’s signature preventive encounter. The Annual Wellness Visit, as currently structured, is still governed primarily by a logic of risk detection and late-stage prevention. CMS deserves credit for building a nationally available, fully covered visit that includes not only traditional preventive elements but also psychosocial risks such as life satisfaction, stress, loneliness or social isolation, pain, and fatigue; review of function and safety; cognitive assessment; referrals to community-based lifestyle and social engagement programs; and an optional social determinants of health assessment. But these elements do not yet define the visit’s central purpose. They remain adjuncts to a framework still oriented mainly toward surveillance, compliance, and the management of downstream risk.
That orientation is increasingly inadequate for an aging society. Older adulthood is not simply a period of accumulating pathology. It is a phase of life in which function, adaptation, contribution, and even improvement remain possible. A recent study by Becca Levy and Martin Slade found that 45.15% of adults age 65 and older improved in cognitive and or physical function over as long as 12 years, and that positive age beliefs predicted those improvements. The policy implication is profound: if later life is framed only as decline to be monitored, our clinical designs may fail to support the conditions under which resilience, growth, and recovery can occur.
The Medicare Annual Wellness Visit should therefore be reimagined. Prevention should remain part of it, but prevention should no longer be the whole story. The visit should become a gateway to late-life health creation: a yearly opportunity to strengthen older adults’ capacity to live lives that are understandable, manageable, meaningful, and socially connected. In other words, CMS should redesign the AWV around a salutogenic rather than merely pathogenic frame.
This is not a call to abandon evidence-based prevention. It is a call to place prevention inside a broader and more humane vision of what health care in later life is for.
What CMS got right — and why it still falls short
Any serious proposal to redesign the Annual Wellness Visit should begin by acknowledging what CMS has already accomplished. The AWV is not empty. It is more expansive than many critics realize.
CMS requires the visit to include a health risk assessment with self-reported information about health status, psychosocial risks, behavioral risks, and activities of daily living. Psychosocial risks explicitly include depression, life satisfaction, stress, anger, loneliness or social isolation, pain, and fatigue. The visit also includes review of medical and family history, current clinicians and suppliers, blood pressure and other basic measurements, cognitive impairment detection, depression risk review, assessment of functional ability and safety, and a written screening schedule. In addition, CMS calls for personalized health advice and referrals to educational or counseling services and community-based interventions aimed at fall prevention, nutrition, physical activity, tobacco cessation, social engagement, weight loss, and cognition. Advance care planning can be included at the patient’s discretion, and the optional SDOH Risk Assessment was added as part of the AWV beginning with the CY 2024 Medicare Physician Fee Schedule changes.
Taken together, these elements amount to a surprisingly promising foundation. CMS has already opened the door to a broader conception of health than many assume. The problem is not that the agency has ignored whole-person care. The problem is that whole-person elements remain subordinate. They are present in the architecture, but they are not the visit’s organizing logic.
That distinction matters. In practice, the AWV still tends to be experienced as a structured checklist encounter. Its center of gravity is the identification of risk factors, the updating of screening schedules, and the documentation of conditions requiring intervention. Even when psychosocial issues are nominally captured, they often do not drive the visit’s priorities, workflow, or follow-up. Loneliness may be screened, but not transformed into a meaningful plan for reconnection. Life satisfaction may be noted, but not treated as a clinically important dimension of trajectory. Community assets may be listed, but not actively mobilized. The result is a visit that gestures toward whole-person care without fully operationalizing it.
This is where a salutogenic critique becomes useful. The question is not whether AWV includes psychosocial variables on paper. It does. The question is whether the visit is designed to create health, or only to identify threats to health. At present, it does the latter far more reliably than the former.
That limitation shows up in at least three ways.
First, the visit remains too biomedically narrow. Even with its broader elements, the dominant clinical question is still, “What diseases can we prevent or slow?” That is important, but it is not the same as asking, “What keeps this person coherent, connected, and capable of living well?” In older age, those are not soft add-ons. They are central determinants of whether medical advice becomes actionable and whether a person can maintain function and purpose.
Second, the visit remains too episodic. The personalized prevention plan often functions as a one-time output rather than a living roadmap revisited across the year. Yet later-life well-being depends on continuity: whether confusion is clarified, supports are strengthened, small actions are sustained, and changes in function or meaning are noticed early enough to matter.
Third, the visit remains too system-centered. Its workflow is largely shaped by documentation requirements, billing categories, and compliance routines rather than by the older adult’s own aims. What matters most to the person in front of the clinician often appears, if at all, as background context rather than as the frame that organizes recommendations.
That is why the AWV, despite its promise, still falls short. It is a good skeleton, but we are mostly leaving it bare.
Why older-adult care needs a new frame: from decline management to health creation
The deeper problem is not just with one Medicare visit. It is with the frame that governs much of older-adult care.
American medicine remains overwhelmingly shaped by a pathogenic orientation. It asks: What disease is present? What risk factors are elevated? What interventions can reduce those risks? That logic is indispensable. No serious reformer should dismiss the importance of blood pressure control, fall prevention, vaccination, medication review, cancer screening, or dementia detection. Older adults benefit from all of these.
But when that logic becomes the only lens, especially in later life, something essential is lost.
A later-life health system organized primarily around decline management is implicitly telling older adults that the main realistic goal is to slow deterioration. It may preserve life, but it does not necessarily support living. It may detect impairment, but it does not necessarily strengthen capacity. It may track burdens, but it does not necessarily activate resources.
The salutogenic paradigm, developed by Aaron Antonovsky, begins from a different question: not only why people get sick, but why some people remain relatively well despite stress, loss, and illness. In this view, health is not a binary state but a movement along a continuum between ease and dis-ease. What matters is not only pathology, but the degree to which a person experiences life as comprehensible, manageable, and meaningful, and the degree to which they can draw on internal and external resources to meet challenges. Your own draft develops this point effectively by arguing that older-adult care should ask not merely what to prevent, but how to strengthen coherence, resourcefulness, and agency in the last decades of life.
This is where the current aging literature becomes especially important. Levy and Slade’s 2026 study challenges one of the most entrenched assumptions in clinical culture: that later life is a unidirectional decline. Nearly half of the older adults in their nationally representative longitudinal sample improved in cognitive and or physical function over time, and positive age beliefs predicted those improvements. Their findings do not mean that aging is easy, nor that frailty and loss are minor. They do mean that our systems should stop treating improvement as an anomaly. Function can improve. Outlook matters. Attitudes toward aging are not merely philosophical; they may shape trajectories.
That insight has direct relevance for Medicare policy. A visit organized around what is likely to go wrong can unintentionally reinforce a deficit narrative. A visit organized around what helps a person remain capable, connected, and purposeful can help create the conditions for a different trajectory. This is not a sentimental argument. It is a clinical and public health argument.
Older-adult care needs, in other words, a more adequate telos. Not simply preventing bad outcomes, but supporting late-life flourishing. That means preserving function where possible, restoring it where feasible, strengthening comprehension where confusion prevails, linking people to supports where burdens overwhelm, and sustaining meaningful roles even in the presence of chronic disease. It means recognizing that an older adult is not only a bundle of diagnoses, but a person still situated in family, community, memory, and aspiration.
The Annual Wellness Visit is the right place to begin this shift because it already exists, it already reaches millions of beneficiaries, and it already contains underused openings for a broader approach. The next step is not to discard it. It is to give it a new center of gravity.
The Salutogenic Paradigm in Policy Language
To make the case for redesigning the Annual Wellness Visit, it is not enough to invoke salutogenesis as an attractive theory. The concept must be translated into policy language: what problem it solves, what it would change in practice, and why it should matter to CMS, clinicians, and health systems.
At its core, the salutogenic paradigm asks a different question than the one that usually governs medical policy. Instead of asking only, “What caused this disease, and how do we reduce risk?” it also asks, “What allows people to remain relatively well — physically, psychologically, socially — even while living with stress, illness, and loss?” That distinction is especially important in later life. Most Medicare beneficiaries are not choosing between perfect health and disease. They are navigating chronic illness, changing function, bureaucratic complexity, caregiving demands, grief, and uncertainty. In that setting, the central policy question is not merely how to prevent another diagnosis. It is how to strengthen the conditions that allow a person to keep living with clarity, capability, and purpose.
Antonovsky’s framework offers two especially useful concepts for this work: Sense of Coherence and Resistance Resources. Your existing draft already translates these constructs into practical design criteria for older adults. Sense of Coherence consists of three linked dimensions: comprehensibility, the extent to which health and life feel understandable and structured; manageability, the sense that one has enough internal and external resources to cope; and meaningfulness, the belief that life is still worth the effort and that continued striving has value. Resistance Resources are the supports that make coping possible. Generalized Resistance Resources include stable assets such as income, literacy, social support, identity, faith, and community belonging, while Specific Resistance Resources are targeted supports for specific burdens: a fall-prevention program, caregiver help, transport services, a grief group, or a reliable neighbor.
In policy terms, these ideas matter because they shift the purpose of the encounter. A pathogenic visit is organized around deficits: what is wrong, what is risky, what guideline should be applied next. A salutogenic visit asks an additional set of operational questions: What helps this person feel oriented rather than confused? What supports make daily life manageable? What roles, relationships, or commitments make health-related effort feel worthwhile? Your draft states this contrast clearly: the dominant model measures blood pressure, A1c, hospitalizations, and polypharmacy, while a salutogenic framing would also take seriously sense of coherence, purpose, social connectedness, functional autonomy, participation, and the experience of care itself.
That is not a softening of medical rigor. It is an expansion of what counts as clinically relevant. If an older adult does not understand their treatment plan, cannot get to appointments, feels abandoned after a spouse’s death, or no longer sees a reason to keep trying, the best preventive recommendations in the world may never become actionable. Comprehensibility, manageability, and meaningfulness are not decorative ideals. They are conditions that shape whether care works.
This is also why salutogenesis belongs in CMS design language rather than remaining at the level of philosophy. Medicare already pays for a yearly wellness encounter. The policy question is whether that encounter should remain chiefly a platform for identifying future threats or become a checkpoint in what your draft aptly calls the late-life “river” — a recurring opportunity to assess where coherence is weakening, where supports are present or missing, and how both clinical and non-clinical resources can be coordinated across time. In this framing, the Annual Wellness Visit becomes less a compliance event and more a coherence and capacity visit: not just a review of risk, but a yearly effort to strengthen the person’s ability to navigate the realities of aging.
Once translated this way, the practical implications become clear. A salutogenic AWV would not discard current preventive elements. It would reorganize them. Instead of beginning with the disease list and ending with a generic prevention printout, the visit would begin with a brief understanding of what matters most to the older adult, take a quick pulse on how understandable, manageable, and meaningful their health feels, and identify key resistance resources already present or urgently needed. Your draft captures this shift well by proposing that Medicare treat each AWV as a navigation checkpoint, explicitly measure and strengthen SOC and resources, and coordinate both clinical and non-clinical supports across years.
The resulting policy logic is straightforward. If CMS wants better outcomes in older age, it cannot rely only on ever more precise detection of risk. It must also support the conditions under which older adults can use care well, sustain function, remain socially connected, and continue to act within lives they experience as worth living. Salutogenesis offers a way to name those conditions, operationalize them, and build them into the most universal preventive visit Medicare already has.
The Hidden Ageism Problem in Current Wellness Policy
If the Annual Wellness Visit is to be redesigned for late-life health creation, one hidden barrier must be named directly: ageism is built not only into social attitudes, but into clinical expectations and policy design. This is not always explicit. No CMS document says that older age is synonymous with inevitable decline. In fact, current AWV guidance includes psychosocial risks, life satisfaction, loneliness or social isolation, function, cognition, and referrals to community-based programs such as social engagement and self-management support. But the dominant logic of the visit still reflects an older assumption: that the main realistic task in later life is to detect losses early, slow deterioration, and manage accumulated risk.
That assumption has enormous consequences. It shapes what gets measured, what clinicians are trained to notice, what patients are invited to hope for, and what kinds of improvement are treated as clinically meaningful. A system organized around decline will tend to ask: What has worsened? What hazard is emerging? What preventive box remains unchecked? Those are important questions. But they are not neutral. They reflect a larger narrative about aging — one in which deterioration is expected, resilience is secondary, and improvement is treated as unusual.
The recent paper by Becca Levy and Martin Slade should be the hinge point for challenging that narrative. In a nationally representative longitudinal study of U.S. adults age 65 and older, they found that 45.15% improved in cognitive and/or physical function over as long as 12 years, and that more positive age beliefs predicted those improvements. Their conclusion is striking: aging should be redefined to include the possibility of improvement, rather than assuming later life is a period of inevitable and universal decline.
For wellness policy, the implication is difficult to ignore. If nearly half of older adults in a national sample showed functional improvement over time, then a preventive encounter designed primarily around surveillance for future decline is working from an incomplete model of aging. And if positive age beliefs are associated with better trajectories, then attitudes about aging are not simply matters of bedside manner or culture-war rhetoric. They are potentially relevant to function itself.
This does not mean that optimism alone reverses frailty, nor that structural illness burdens can be wished away. It does mean that clinical frameworks carry psychological and behavioral signals. When the most universal Medicare wellness encounter treats older adults mainly as people to be screened, warned, and managed, it risks reinforcing a self-understanding centered on vulnerability alone. By contrast, a visit that explicitly recognizes the possibility of adaptation, reserve, contribution, and even improvement may support a different orientation — one in which the patient is not merely bracing for loss, but actively investing in capacity.
The broader public health literature strengthens this point. The World Health Organization describes ageism as the stereotypes, prejudices, and discrimination directed at people based on age, and notes that it has serious consequences for health and well-being, including poorer physical and mental health, slower recovery from disability, increased social isolation and loneliness, and lower quality of life. WHO also notes that ageism can be institutional, interpersonal, and self-directed. That last form — internalized ageism — is particularly relevant here. A wellness policy can unintentionally convey a worldview in which old age is defined by what can no longer be done. Once absorbed by patients themselves, that message may dampen effort, narrow expectations, and subtly erode the sense that life remains open to growth.
Seen this way, the problem with current wellness policy is not simply that it omits positive language. It is that it often embeds a deficit template into routine care. The Annual Wellness Visit does ask about life satisfaction, loneliness, fatigue, function, and cognition, but these are generally treated as risks or symptoms to catalog rather than as dimensions of a larger human trajectory that can worsen, stabilize, or improve. The visit is still better at naming vulnerabilities than at cultivating the resources that help older adults move in a healthier direction.
A salutogenic redesign would not deny the realities of aging. It would reject only the assumption that those realities exhaust the story. Levy and Slade’s findings give policy makers permission — and perhaps an obligation — to build Medicare encounters around a fuller anthropology of later life. Older adulthood should not be approached only as a zone of loss prevention. It should also be approached as a stage in which people can strengthen coherence, deepen connection, reclaim function, and remain meaningfully engaged.
That is why the ageism question belongs at the center of AWV reform. The redesign challenge is not only technical. It is moral and conceptual. What kind of aging does Medicare imagine when it sends millions of people into a yearly “wellness” encounter? If the answer is mostly a future of anticipated decline, then even a well-intentioned preventive benefit may undershoot what older adults need. But if the answer is a future in which well-being, function, and purpose remain open to cultivation, then the Annual Wellness Visit can become something more than a checklist. It can become an instrument for changing trajectories.